


COVID FAQ Summer 2021, Part 1

You shared the last article about the Delta Variant so much that nearly 400,000 people read it. Thanks for spreading the word on something so important. You also asked so many good questions that I have tried to answer as many as I could in this article.
It’s so long that I split it in two pieces. This 1st piece covers these questions:
1. What’s the Update on the Delta Variant and Cases Worldwide?
2. Am I Safe If I’m Vaccinated? What Activities Can I Go To? Why Are There Still Cases in Very Vaccinated Countries?
3. I’m Vaxxed. Can I Go to an Indoor Event if I Get Masked?
4. When Will We Leave This Behind? When We’re All Vaccinated?
5. Can Vaccines Stop the Pandemic?
6. Do We Know More about Vaccine Effectiveness?
7. Should Vaccines Be Fractionalized?
8. Should I Get a Booster Shot?
9. Should I Mix-and-Match?
I’ll send the 2nd piece tomorrow for premium members. It covers these questions:
10. What Are the Side Effects of the Vaccines?
11. Does It Make Sense for Some Groups to Not Get Vaccinated Then?
12. Should We Have Mandatory Vaccines?
13. How Should We Deal with Immunocompromised People?
14. Why Did Cases Go Down in India? What Really Happened There?
15. Should We Attempt Complete Elimination of COVID?
16. I Want to Travel to Europe/America. Will I get Locked Down?
17. Does Ivermectin work?
18. It Looks Like Most of Us Will Catch COVID Anyways. Vaccines Reduce the Risk. Why Wear Masks?
I’m hoping to post soon an article about Long COVID and another one about kids. Subscribe if you want to receive them!
1. What’s the Update on the Delta Variant and Cases Worldwide?

The virus has kept spreading in many countries. In some, like the UK, Portugal, or Spain, cases are still very high, but new daily cases are lower than at the peak. But in the UK, for example, it doesn’t look like the virus curve is about to go all the way down.
Why are cases already going down in some countries but not others? At this point it’s really hard to tell. There are too many confounding factors. Some regions might have gotten close to herd immunity through vaccines, infections, or both. Since it’s August, many people in Europe might be taking holidays, which means more time outside, which is good for avoiding the virus. Or they’re traveling, so they’ve been extra cautious. Or they’ve avoided getting tested. Or maybe it’s the mitigating measures that have appeared in some places. Maybe people started masking up again due to Delta fears… Probably it’s a mix of all of the above, and yet some other factors.
So what’s the deal? This gif might give us a good sense. It’s the incidence across European regions from the end of June to August 7th 2021:

Last year, we had to wait until September to see this level of contagion.
With all these mixed evidence, how do you get a reality check on how bad Delta is? By looking at countries that have had few infections since the beginning of the pandemic.

Thailand and Japan, for example, have been able to keep the virus at bay for over a year, but with the same processes and 20%-50% of their population vaccinated, they are now facing historic peaks.
To me, this is a sign that Delta does indeed spread much faster, and that countries with low vaccination rates will have a hard time, especially once Fall comes around in the Northern Hemisphere.
However, the fact that case numbers went down quickly in some countries is also a sign that we can beat the virus, as long as we vaccinate enough people and remain careful. It’s probably not a coincidence that Portugal, Spain, and the UK have caseloads going down: all three have over 70% of the population vaccinated—and probably a sizable share of the rest recovered from infection. They might be close to Herd Immunity.
2. Am I Safe If I’m Vaccinated? What Activities Can I Go To? Why Are There Still Cases in Very Vaccinated Countries?
There are still cases in highly vaccinated countries because not enough people are vaccinated—and maybe also in part because of breakthrough infections.
For example, let’s take a region where two thirds of people are vaccinated. Let’s assume 20% of the population caught the virus in the past1. That means close to 75% of the population has some sort of immunity.

Now let’s assume immunity through vaccination or previous infection reduces the probability of new infections by 60%. The transmission rate for the immune group is thus 60% lower. For the overall population, it’s 45% lower. It’s still 0% lower for those not immune.
If R0 for Delta is 62, a reduction of 60% means every infected person now infects ~2.5 people instead—on average. If you further add summer outdoors activity and masks, you easily get below 1 and stop the spread.

But averages don’t capture what happens in reality. A group formed of unvaccinated people still has an R of 6.

For example, the 25% of people who are not immune yet might include lots of young people. If 1000 people between 18 and 30 gather in an indoors party unmasked, and most of them are still at risk, that will be a superspreader event, and the caseload will explode.

Even with mostly immune people, this might still be a superspreader event if it’s indoors and unmasked. The more outdoors the event is, the more ventilated, the more masked, and the more vaccinated, the lower the likelihood of creating a superspreader event and catching the virus.
All of this is for catching the virus though, not for having serious consequences. If instead of R we look at the likelihood of dying (Infection Fatality Rate, IFR), this changes.
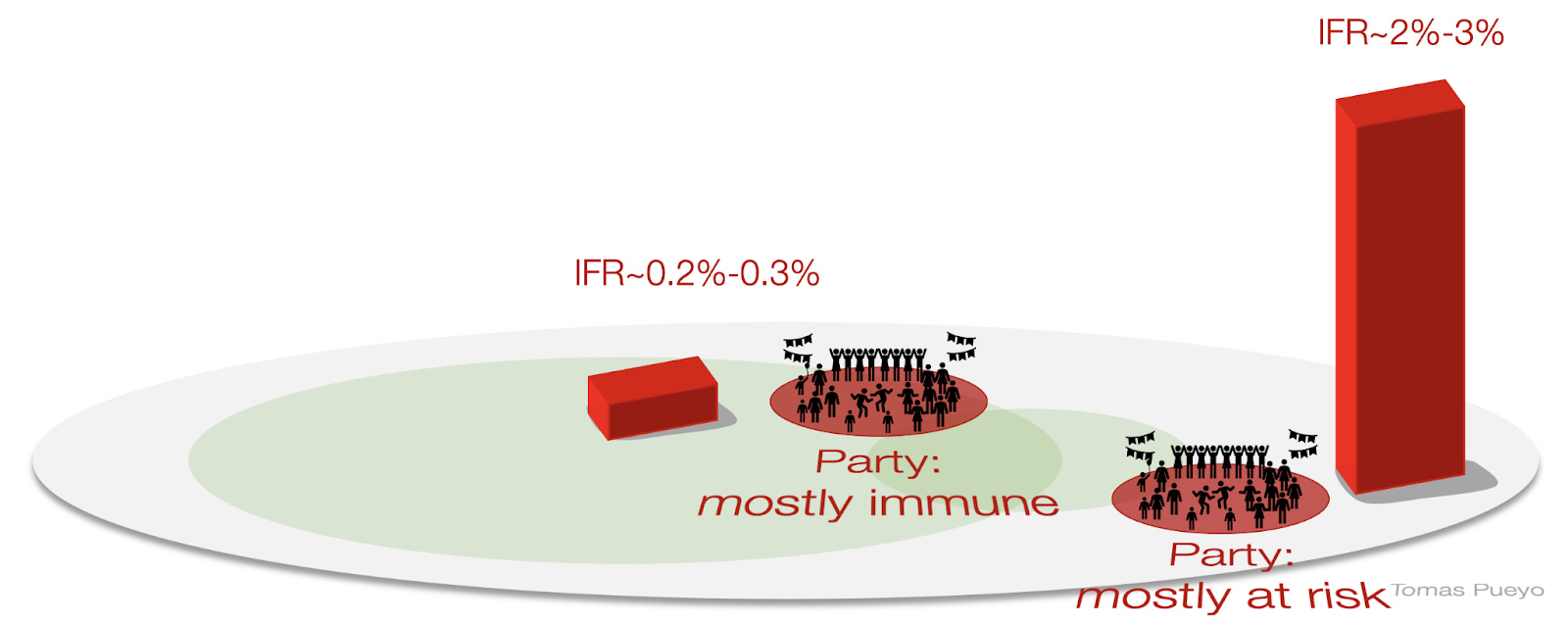
If you catch the virus in the mostly immune party and you’re vaccinated, your likelihood of death is ~0.2%-0.3%, but 2-3% if you’re unvaccinated—on average.
If you’re 40 years old and vaccinated, your likelihood of dying if infected is about 0.01%. Without a vaccine, it’s ~0.1%. In both cases, quite low.
The question becomes Long COVID: if you’re unlikely to die going to such a party, but you can get a chronic condition from it, would you still do it? I’m looking into Long COVID right now and hope to publish something on it soon.
3. I’m Vaxxed. Can I Go to an Indoor Event if I Get Masked?
From the previous question, you can see that the R for vaccinated and masked people might be around 1. The key variable is the environment. The risk of catching COVID is higher if:
You are surrounded by unvaxxed people.
There are thousands of people at the event.
People come and go.
Ventilation is poor.
People talk.
People sing.
People are cavalier about properly wearing masks.
You’re older.
There’s a high prevalence in the area.
For example, a cinema with 50 spots to watch a 1h30 movie in an area that has a high vaccination rate and low prevalence will be safer than a 3-day event with 100,000 people singing and talking in indoors and outdoors settings.
If you don’t know some of these details for the event, ask the organizers about the setting. The more they can answer, the better. And if they don’t know these details, they probably don’t care, which means they don’t take safety seriously, which is another data point to consider.
4. When Will We Leave This Behind? When We’re All Vaccinated?
It depends on what you mean by “leave this behind”.
If we’re all vaccinated, remember that the transmission rate only goes down by ~60%. So if we release all measures and R0 f Delta is ~6, the R will still be ~2.5 with everybody vaccinated. It will still run through the population :/
However, when it does, it won’t cause that much havoc. With only ~0.2% of people dying, it’s close to a terrible flu season, so it might be tolerable.
We might, then, reopen everything with no limits… Unless Long COVID is super bad, which I hope to know in a week or two (subscribe!).
From all of this, I think the most likely scenario is that we keep vaccinating people, others get natural immunity, we keep masking up, we keep avoiding the worst type of superspreader events, most other events are open, and society keeps chugging along for months.
That is, unless vaccines solve this problem.
5. Can Vaccines Stop the Pandemic?
Yes.
Imagine that we could produce tens of billions of vaccine doses every year, approve them within weeks of a new variant appearing, and distribute them across the world. The effectiveness of such a vaccine might go to 95% to prevent infections, which would reduce R to way below 0, stop the pandemic, and also stop the quick mutation of the virus.
This is doable. Look at this beautiful graph:

Within 8 months, we’ve gone from 0% to 30% of the world population vaccinated. How beautiful is that? It’s a testament of what mankind can do with the proper coordination system (in this case, capitalism with some state intervention).
If the mutation is slow enough, and vaccination reactivity fast enough, we might be able to nip new variants in the bud, and either eliminate COVID or limit it to pockets of unvaccinated/immunosuppressed people.
The wild card here is animals: if the virus can jump easily to other species where it can spread, mutate, and then jump back to humans, we might not be able to stop it. We know such jumping has happened in the past, but I don’t know how likely this nightmare scenario is at scale.
6. Do We Know More about Vaccine Effectiveness?
Lots of people have asked me about the “true effectiveness of vaccines”, but that number doesn’t exist. It depends on many factors: what vaccine you got, how many doses, how much time between them, what variant we’re talking about, how old you are, what countries the data comes from, how representative the sample is, etc. That’s why I gave broad numbers of about ~50% reduction in symptomatic infection, and ~90% in reduction of hospitalizations and deaths.
One update we’ve had since the Delta article came out is from the UK, where the updated effectiveness of vaccines is of ~50% reduction infection, and 60% reduction in infection with symptoms. Prevention of hospitalization or death is still ~90%.
Another update just came today from a study by the Mayo Clinic, looking at the mRNA vaccines of Moderna and Pfizer. According to it, Delta is still good to protect against hospitalization and death, but it reduces infection risks by 75% for Moderna and 40% for Pfizer. This might be one of the reasons why Israel is suffering more than the UK.
Honestly, at this point, I think we’re paying too much attention to updates on current vaccine effectiveness (we know the broad order of magnitude: about 50% protection from infection, about 90% from serious consequences) and not enough to the speed of releasing new vaccines.
For example, Novavax appears to have 90% efficacy, including against new variants, and has milder side effects. It might be the best one yet. Updates to the mRNA vaccines to fight the new variants are also sorely needed. Let’s make these happen.
7. Should Vaccines Be Fractioned?
An interesting paper3 says there have been some tests in the lab—and one in real life—and it looks like half a dose is nearly as good as a full dose. So we probably should fraction vaccines. Definitely in the emerging countries that can’t get enough of them. But also in developed countries if the surplus could accelerate local vaccination rates or international ones.
8. Should I Get a Booster Shot?
I don’t know. We enter into the domain of speculation here. But we should speculate, because we’re making decisions with little data, whether we want to or not. Making no decision is making the decision of doing nothing.
It does look like the protection of shots wanes, but it’s not clear why. It’s probably because of two reasons: the appearance of new variants and the simple passage of time4. My speculation is that it’s more linked to new variants than simple time waning5, but both can be considerable.
That means a new booster shot of the same vaccine might help a bit, especially if you were vaccinated a very long time ago. But what will really make a difference is an updated vaccine that covers new variants.
Short of that, a booster shot from a different vaccine might be better than using the same vaccine6.
9. Should I Mix-and-Match?
According to the WHO, you shouldn’t.
I humbly think the WHO is wrong.
And you can tell by paying attention to the details of what they say.
"[The WHO] advised individuals against mixing and matching COVID-19 vaccines from different manufacturers, saying such decisions should be left to public health authorities." (bolded mine)
Note how they don't say it's bad for you. They say individuals shouldn't make a decision on it. Why? Here:
"It will be a chaotic situation in countries if citizens start deciding when and who will be taking a second, a third and a fourth dose."—Soumya Swaminathan, WHO Chief Scientist.
Her concern is not that mix-and-match doesn't work! It's about political and logistical chaos!
In fact, it's the opposite. Mixing and matching is easier logistically than ensuring that people get jabbed with the same vaccine: you don’t need to have the same vaccine at the right time for the right person, which makes scheduling and inventory management far easier.
She also mixes number of boosters with mixing-and-matching. Then she adds:
"Data from mix and match studies of different vaccines are awaited—immunogenicity and safety both need to be evaluated."
So she is either not knowledgeable about the data that exists, or doesn't incorporate the new data to make early decisions7. This is exactly the type of mistake the WHO has made in the past, waiting for a golden standard of evidence without accounting for the cost of time amidst an ongoing pandemic.
Then the article mentions the WHO does, in fact, advise mix-and-match in some situations!
"The WHO's Strategic Advisory Group of Experts on vaccines said in June the Pfizer Inc (PFE.N) vaccine could be used as a second dose after an initial dose of AstraZeneca (AZN.L), if the latter is not available."
The WHO was late on declaring this a pandemic, on supporting masks, and they still don’t acknowledge aerosol transmission at this point8. So we need to be critical of what they say now, too. Unfortunately, it looks like their processes are failing again this time.
So what do we really know? Based on the information available today, we should indeed mix vaccines.
We have to realize that the only reason why we mandate 2 doses of some vaccines is because that's what we tested, and it turned out to work.
It doesn't mean 2 doses is ideal.
It doesn't mean that amount is ideal.
It doesn't mean 3 weeks apart is ideal.
The question then is: what is ideal? We can't test all combinations with randomized controlled trials (RCT), which are the gold standard in science. It's hard enough to just test vaccines.
Instead, we can rely on priors and improve them with new evidence. What’s our prior?
The world is messy. The variants present during a RCT are not all the variants people will face. Things evolve. Which combination do you think will be more effective: one that prepares you to fight the exact same enemy twice, or one that shows you different enemies?
The more diverse your enemy, the more your body can learn to fight a generic enemy rather than a specific one. So the prior should be that mixing vaccines is better than getting twice the same vaccine.
This intuitive prior was already tested in the past, and the evidence on COVID is showing that mix-and-match gives more protective antibodies.
As for the risks, mix-and-match doesn't appear to lead to more hospitalizations or deaths. It does make people feel worse, which might be an indication that the immune system is working overtime. What we know empirically about risks confirms what our priors would tell us to expect.
Finally, the immune response has been tested in labs in at least 3 studies, and it appears to be very slightly stronger with mix-and-match than without. Here’s the translation for one of them:

For all these reasons, many countries already allow it: Canada, Spain, France, the UK, Germany, Italy, Sweden, South Korea...
If you're interested in learning more and keeping up with the latest data, search for "heterologous prime-boost".
Summarizing:
Mix-and-match is probably not more dangerous.
It’s probably slightly better for immunity.
Logistically it’s easier to allow it.
Therefore, it should be allowed.
I hope you enjoyed this! The second piece is tomorrow. I will also soon write about Long COVID and about kids and back to school in the fall. Subscribe if you’re interested!
Also, feel free to comment. There were so many questions here that I couldn’t research them all perfectly. I’m sure I’ve made mistakes.
Let’s respect the Rules of Engagement. The questions you guys bring up are really great. Thanks for being such an intelligent group of people. Please bring in your comments, questions, and disagreements! As long as you respect the following rules, I will respond to the best of my knowledge:
Please specify what you disagree about.
When you make a statement about a fact, please add a link.
Be cordial. I’m not always right, and I’m happy to identify my mistakes to correct them.
Disagree about the data and arguments, never about the person. Avoid ad hominem attacks. I will immediately ban you and delete your comments.
And that vaccination and previous infection are independent.
How many contagions are caused by an infected person, if there are no measures and there’s no herd immunity. Ie, one person infects 6 other people if there are no measures and nobody is vaccinated or immune through having caught an infection earlier on. This comes from the Delta article.
Thanks to Tom Raggett for the Twitter thread that led me to the paper!
Why can we assume this? First, we do know that new variants reduce efficacy because of how fast Delta has reduced efficacy in a country like the UK.. But how can we know that the passage of time also reduces vaccine efficacy? Because we know AstraZeneca (primary vaccine in the UK) had originally a lower efficacy than Pfizer (primary vaccine in Israel), but Israel—which vaccinated earlier than the UK—has a lower vaccine efficacy than the UK. Assuming both have been similarly exposed to Delta, the only way vaccine waning could be stronger in Israel than in the UK is due to the passage of time.
The reduction in efficacy between Israel and the UK (which we can assume is due to time) is not huge, and the data is noisy, so we can assume the time effect might not be massive).
This is advice for you as individuals, not for governments. Governments should weigh the global value of a booster shot to their population vs. increasing the speed of vaccinating the world. So if governments decide a booster shot is not ideal for this reason, and it’s properly analyzed, I’d be ok with that.
My guess is the latter, since the WHO tends to be very up to date on what’s going on, but refuses to incorporate partial data.
I understand why they don’t: it’s hard to find the actual virus in the air, and many tests haven’t been able to reproduce aerosol infections in a lab. But in real life, we’ve seen too many instances that can be best explained by aerosol infection, that the right thing is to assume it’s happening while we wait to understand the science better. For centuries, we believed in Newton’s gravity. Even if it is bogus, it is a very useful model of reality. So is it for aerosol transmission.
Whether booster shots should be allowed is the wrong question. We should be asking whether they should be offered in highly vaccinated populations while there are still so many countries with low or no access to vaccines at all. For pharmaceutical companies, selling boosters in developed countries offers greater profits faster than selling first and second doses in developing countries. Global public health policy should not be dictated by the pharmaceutical investors' desire for greater dividends, but by global public health considerations.
There simply does not appear to be a pressing public health need for booster shots. Easily detectable T-cells and antibodies reduce over time, but there is no reason to believe that immune response (whcih is to say immune memory) disappears along with them. Meanwhile, in many countries, vaccination rates are still so low that capacity does not even meet the needs of front line health workers treating COVID patients, let alone vaccinating at-risk groups.
This is not only a moral failure, it also provides perfect condidtions for the emergence of new variants. Instead of deepening protection in highly vaccinated countries by diverting capacity to booster doses, we should we widening coverage to more countries in order to run as fast as we can towards global herd immunity. Only then will we really be able to learn to live with the virus.
Me asombra que el aumento de casos en Israel lo quieran resolver con una tercera dosis y sigan sin inmunizar a los palestinos que necesitan a diario para hacer los trabajos que ellos no quieren y por lo tanto entran y salen de Israel y pueden contagiar. No he visto recientemente ningún artículo que hable de esto ni el porcentaje de vacunados entre la población palestina. Creo, aunque puede que me equivoque, que aunque nos pongan 10 dosis si llegan personas sin vacunar a nuestro entorno, voveremos a contagiarnos. Gracias por el artículo y los enlaces y referencias. Interesante para mi la vacuna Novavax