
The Most Alarming Problem about Long COVID
It's Probably Chronic Fatigue Syndrome

The main problem with Long COVID is its complexity: dozens of symptoms, different causes, different treatments, vaccine protection, Delta variant, age impact, gender impact, evolution over time…
This complexity is crippling. We think “Hmmm Long COVID is bad but how bad? I don’t know… Maybe we should avoid it? But how careful should we be? I don’t know. Is it worth keeping masks? Staying indoors? I don’t know...” So how can we simplify things?
By looking at the most alarming problem that Long COVID most likely causes: Chronic Fatigue Syndrome. There are other problems, such as unregistered deaths, post-intensive care syndrome, chronic loss of smell... But they’re too much, and I don’t think they change our takeaways, so we will look at them in the premium deep dive this week, along with other things.
So today you’ll learn:
What’s the worst aspect of Long COVID?
How long does it last?
What are your odds of catching Long COVID?
What causes it?
Can we treat it?
Ok let’s go.
Is Long COVID Like Chronic Fatigue Syndrome?
One of the main issues with Long COVID is that it’s a long-term illness, but COVID hasn’t been around for a long time, so we don’t know what happens in the long term. How can we know what COVID will be in a few years?
What if there was an illness that looked a lot like the main outcome of Long COVID? We could see what that looks like and how it evolves over time, and make an educated guess on what will happen with Long COVID next.
That’s what Chronic Fatigue Syndrome (CFS) is: an illness that seems a lot like the typical long-term outcome of Long COVID, and for which we already know a lot, since it affects between 1 and 2.5 million Americans.
For example, this is Jessica. I highly encourage you to watch these videos. They don’t need sound. You can’t get a sense of Long COVID if you don’t watch them.
Jessica has had CFS for over a decade now. She’s bedridden. Putting her feet on the ground is enough to knock her out.
This is TED Speaker Jennifer Brea, suffering here from post-exertional malaise episodes, a typical symptom of CFS where a very small effort can knock you down for weeks. In this case, she cheered from her wheelchair.
Jennifer is the producer of Unrest, a documentary that you can watch on Netflix (trailer). All of these clips come from her documentary.
Whitney has not talked for years. According to his father, Ron Davis:
“Whitney’s state is comparable to an AIDS patient about a week before his death. And that has been the case for the last six years.”—Ron Davis, Whitney’s father, Al Jazeera.
“This is a devastating, really serious disease that affects many body systems. It will completely knock you out, it will ruin your life and the lives of people who take care of you. It can affect anyone if they just get the wrong virus or the wrong environmental stress.”—Janet Dafoe, Whitney’s mother, Al Jazeera.
More and more, it looks like the most alarming illness of Long COVID is indeed CFS. According to Fauci, “a considerable number” of COVID survivors struggle with extreme exhaustion, memory lapses, and cognitive difficulties many months after they have been officially cleared as “recovered”. This sounds exactly like CFS.
Here’s an example of a Long COVID patient: Caitlin, the 28 year-old dietician who used to run for two hours every day, had COVID with mostly cold-like symptoms, and one year later is now almost completely bedridden:
“My symptoms change all the time. I’m happy if I can take a shower.”

“She struggles to brush her teeth or prepare meals, because her heart races to 180 beats a minute. (A typical rate is 60 to 100.) Convulsions sent her to the emergency room in September. She is alone most of the day—her husband works long hours—and she has to plan carefully in order to use the bathroom and feed herself without collapsing.”—Meghan O'Rourke,The Atlantic
This definitely looks like CFS. Like the stories of so many other people who have developed Long COVID.
How is it possible that Long COVID leads to the same outcomes as CFS? Because CFS usually happens after viral infections, including ebola, Epstein-Barr, HPV, Lyme (bacterium in this case), Dengue and, interestingly, the flu and SARS.
“Most well-studied viral or bacterial pathogens have been connected to the development of chronic symptoms in a subset of infected patients.”—Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms, Amy D. Proal and Michael B. VanElzakker.
How long does that last? You’ve probably noticed the worst part of CFS: it’s the word chronic.
How Long Is Long COVID’s Chronic Fatigue Syndrome?
We don’t know yet, because little time has passed. But we can look at two data points:
Analogies: how do people evolve from traditional CFS?
What’s the trajectory of Long Haulers (those with Long COVID)?
1. Analogies with CFS
Many people suffer from CFS for decades.
The SARS experience is one of the most frightening given the COVID virus is from the same family:
“One team studied 233 SARS survivors approximately 4 years after initial infection, and found that 27.1% met the [...] CDC criteria for chronic fatigue syndrome.”, Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms, Proal and Van Elzakker.
In general, only 5% of those with CFS ever return to normal.
So what we know about CFS is not good for the long term. What about current COVID Long Haulers?
2. Trajectory of COVID Long Haulers
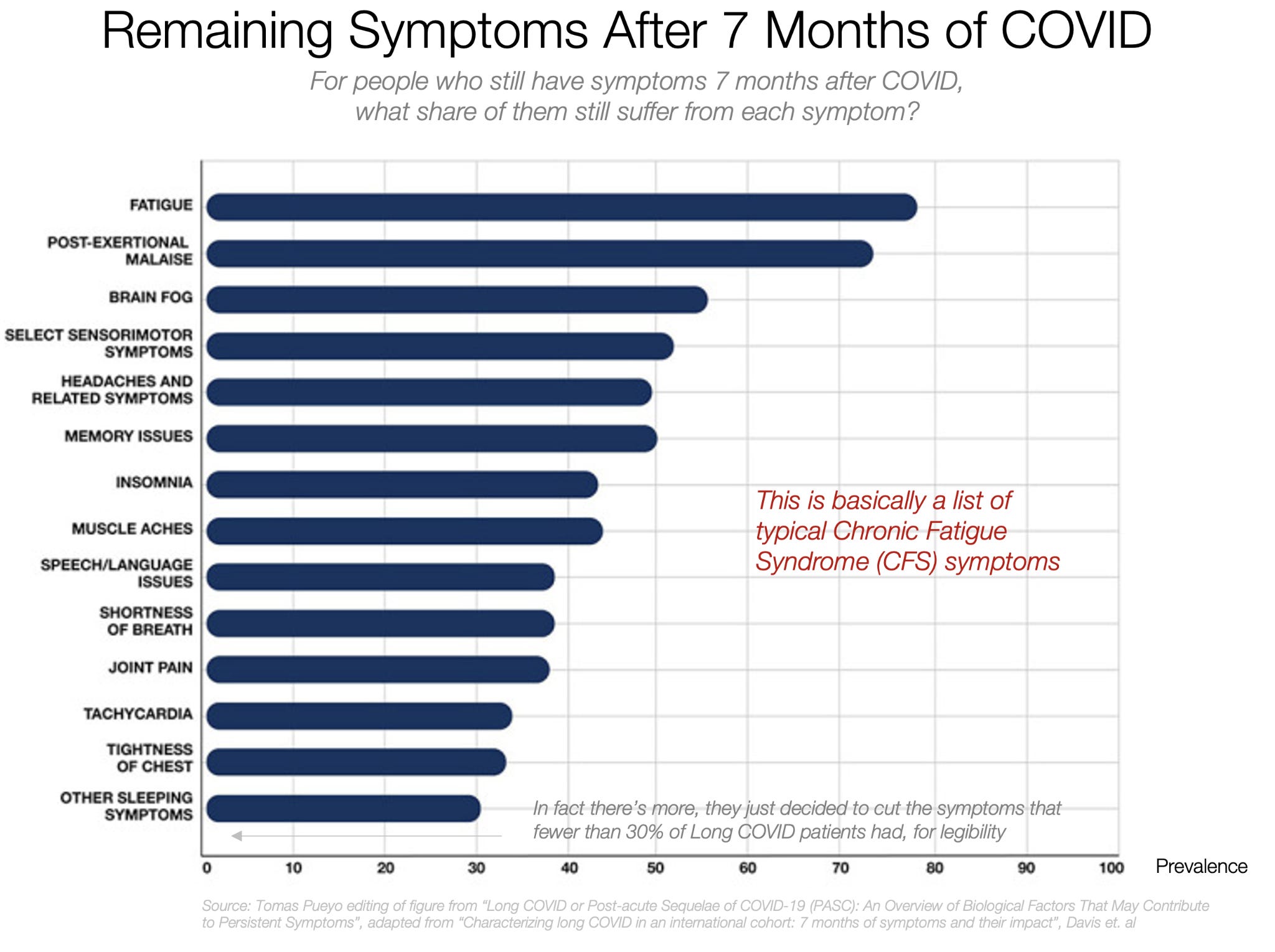
One study from English healthcare workers shows these symptoms 6 months after infection.

Long COVID has many symptoms. Those lasting 6 months or more are the same as the symptoms of CFS. As you know, we don’t have much more than that for COVID. But what’s the trend?

It flattens out substantially as months pass by.
Most studies I have seen show broadly the same thing. 10% of those who tested positive for COVID in an Australian clinic had not recovered from Long COVID after 8 months.
Even following mild courses of COVID, 11% of patients in another study still could not fully participate in everyday and work life 7 months after disease onset.
Maybe the symptoms that are more like CFS tend to be the ones disappearing the fastest? Nope.

The opposite is true: the CFS-like symptoms are the most common and the longest-lasting.
A lot of this data is self-reported, because we can’t find CFS with lab tests. Is there anything more objective we can use to quantify how all of this evolves over time? Like heart rate while resting?

If the evolution of the heart rate is any indication, and this continues in the coming years, this might indeed be a chronic condition.
So summarizing here: it’s very possible that about 10% of those who catch COVID develop some sort of CFS and they don’t recover.
How crippling is it?
How Does Long COVID Chronic Fatigue Syndrome Affect Your Lifestyle?
It can destroy it.
You’ve seen the stories above, but how common are they?

If you catch Long COVID, there’s an 80% chance it will affect your ability to work, and in 40% of cases your finances will suffer. From other studies, 60% say they’re somewhat limited, and 20% say they are limited “a lot”—which often means being unable to do even a part-time, desk-based job.
So about 10% of those who get COVID will have Long COVID.
And about ~20-30% of them say it’s crippling.
Therefore, our best assumption should be that about 2-3% of those who get COVID will have a crippling Long COVID similar to CFS. Two similar analyses from people I respect find the same thing.
Who does it impact most? Old men, like COVID deaths? Again, no.
Who Gets Long COVID’s Chronic Fatigue Syndrome?
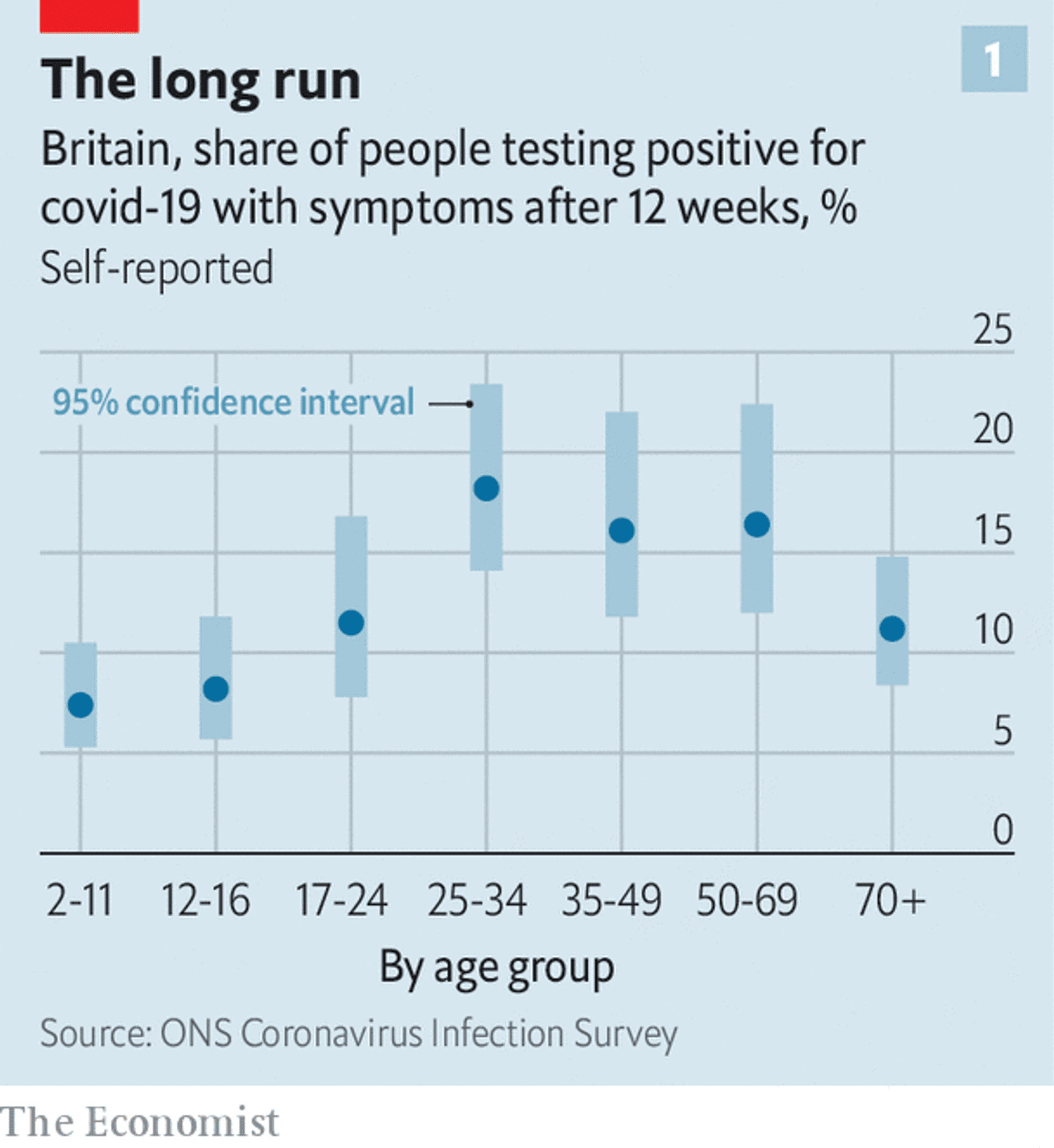
The majority of Long Haulers are working age, at a rate of nearly 20% of those who test positive!
What about young kids? They have the least Long COVID, but it’s only 2-3 times less likely than for 25-34 year-olds. According to this paper and this paper, the likelihood of developing Long COVID in kids is at most ~5%. Which is concerning to me as a parent. 5% is a lot. With 4 kids, the chance that one of them develops CFS from COVID becomes 20%1.
Again, this is for all Long COVID, not just the CFS cluster (I couldn’t find data on that). But it’s possible that the distribution is similar for COVID CFS2, since:
That’s what it looks like for all Long COVID symptoms
It’s also what it looks like for CFS.

The other thing we know about CFS is that women suffer from it more than men.

It appears that this is broadly true for Long COVID too: a Parisian hospital had 4x as many women as men with Long COVID, another study identified women as more likely to become long haulers, and this one, and this one from Mayo Clinic...
So standard CFS and COVID CFS are both post-viral illnesses that impact about the same ages and the same genders with the same symptoms. It really looks like a big chunk of Long COVID patients simply have CFS.
Thankfully, we have vaccines. They reduce infections, hospitalizations, and deaths. Surely they reduce Long COVID’s CFS too?
Can Vaccines Prevent Chronic Fatigue Syndrome from COVID?
Yes! Finally some good news.
We know from Delta variant research that vaccines halve your likelihood of catching COVID. But once you do catch COVID after a vaccine, what’s your likelihood of developing Long COVID?
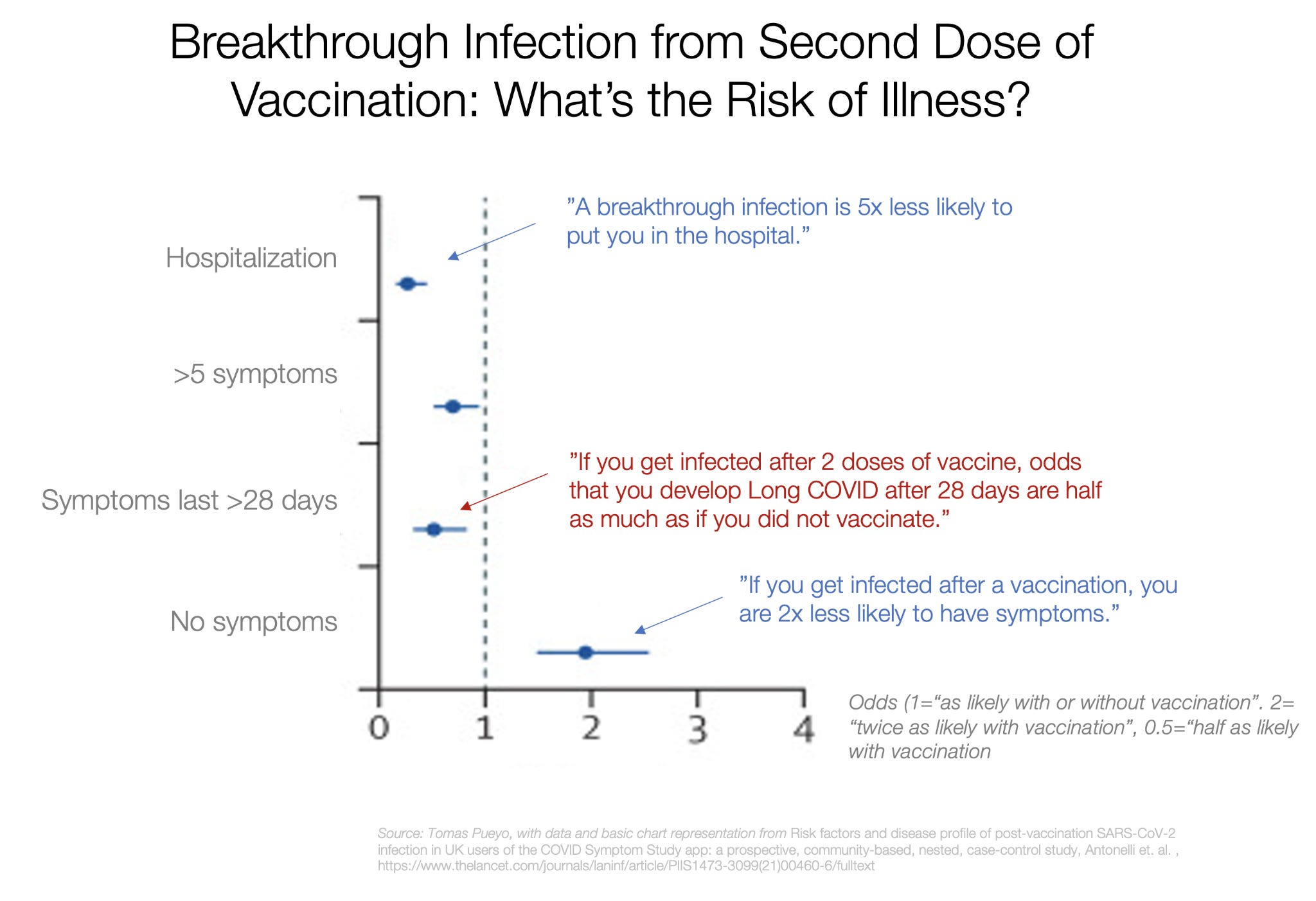
It looks like after 2 doses of vaccine, if you do have a breakthrough infection, the likelihood of having symptoms 28 days later is about half. This is true across the board for all symptoms:

This paper found the same thing, whereas this other paper found that 20% of healthcare workers with a breakthrough infection had symptoms after 6 weeks.
Assuming this difference continues over time, it might mean that vaccines reduce your chances of catching CFS from COVID by ~75-90% (50% reduction in likelihood of infection, and 50-80% reduction in long-term symptoms after a breakthrough infection). If they were 2-3% without vaccines, the odds of developing CFS with a vaccine become ~0.2-0.75%.
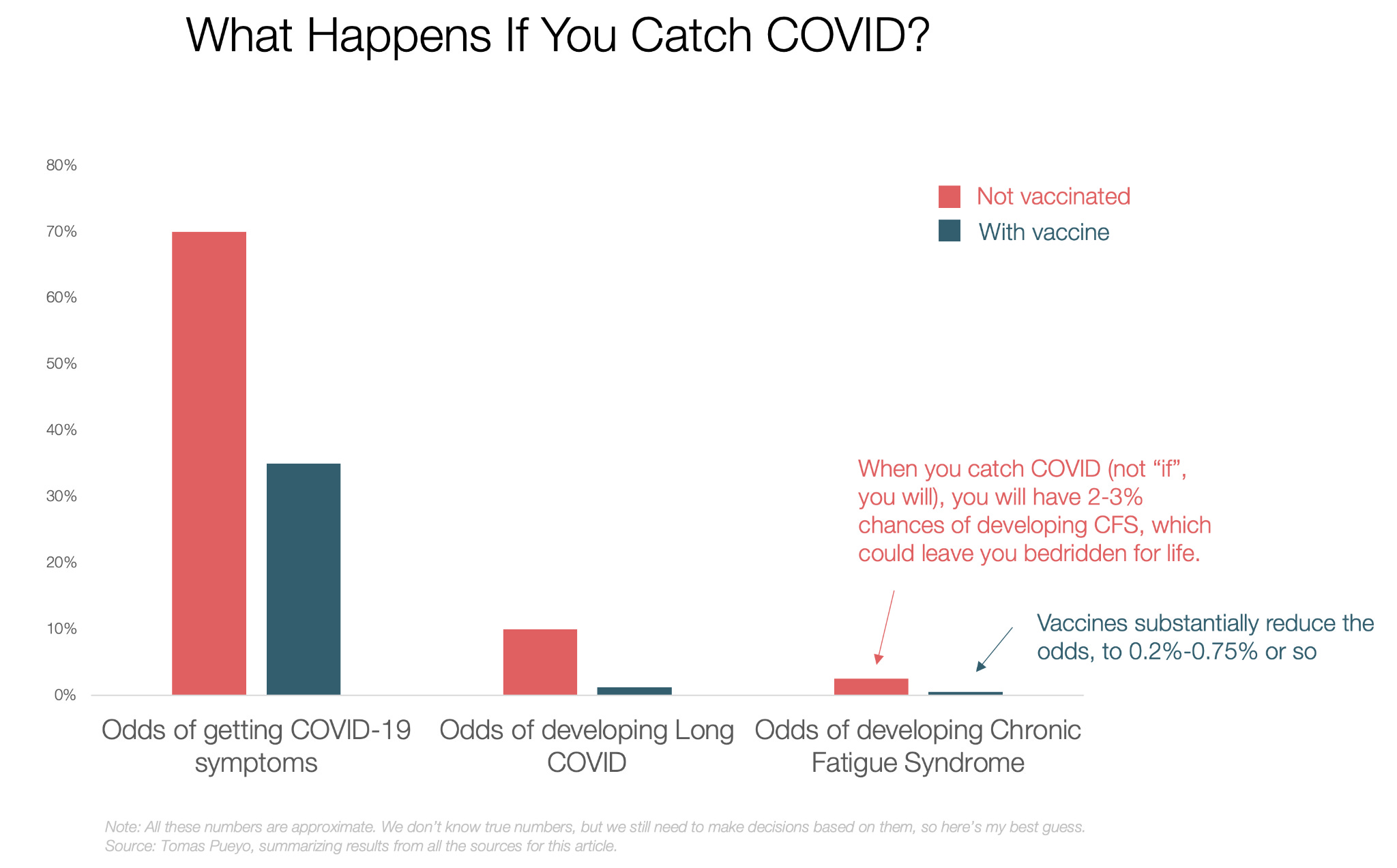
This is only an approximation: all these numbers will change so much based on the population’s gender, number of vaccine shots, type, time since vaccinations, variant of infection, previous infections, genetics… What we care about are the orders of magnitude. What we’re saying is the odds of catching CFS without vaccination are about the same as dying from Delta—except CFS is for all ages. And vaccines dramatically reduce that likelihood.
It’s not the only benefit from vaccines. They can also help relieve some CFS.
Apparently, about 30-40% of Long Haulers report an improvement in their symptoms after being vaccinated. It doesn’t cure the symptoms, and we’re not sure how long that relief lasts, but at least it looks like it helps some of them. How can that be?
To answer that question, we need to understand what might cause CFS in Long Haulers.
What Might Cause CFS in Long COVID?
There are three main hypotheses on why these symptoms last so long:
The COVID-19 virus (or other equivalent viruses for other CFS) survives inside the body forever, pushing the immune system to chronic alert level.
The immune system becomes dysregulated, and stops fighting another set of viruses, which now are more free to roam and affect the body, which the immune system then needs to fight in a chronic war.
A dysregulated immune system attacks the body itself. In this case, it would be an auto-immune disease.
There is evidence for all 3, across both Long Haulers and patients with other types of CFS. Tests have found in the blood remains of viruses and high levels of antibodies.
I started going down this rabbit hole, but I stopped when I saw the complexity of the disease and how little we still know about it.

So we’re not sure what causes CFS, but here again, the parallel between CFS in Long COVID and outside of it is pretty evident.
Can We Treat CFS in Long COVID?
The bad thing about CFS is that, as far as I can see, it can last forever and has no proven cure.
Let that sink in.
Some interventions might alleviate symptoms for some people, but that’s it. For example, magnesium injections, dry environments, or a drug under research called Ampligen3.
Many times, it makes it worse. For example, physical rehabilitation might knock out CFS patients and reduce their resilience over time.
This is probably why the #1 cause of death for CFS patients is suicide: so many of them hate seeing life pass by while they’re locked inside their body...
In COVID statistics, you’re either dead or alive. But if you have CFS, are you fully alive? Or something in between4?
Takeaways
The big takeaway is that there’s a high likelihood that the worst part of Long COVID is Chronic Fatigue Syndrome. We can’t be 100% sure, but it looks like it, it smells like it, it tastes like it, and it sounds like it. Like traditional CFS, COVID CFS:
Has the same symptoms.
Also appears after a viral infection.
Also affects women more, especially in their fertile years.
Also seems to be caused by a combination of remaining virus and immune system gone awry.
This parallel is important, because if it’s indeed true, it means COVID CFS
Would be chronic.
Has no known cure.
And many people commit suicide because of CFS.
What’s your likelihood of developing it? About 2-3% of all unvaccinated people who get COVID will probably develop COVID CFS. This is true at all ages, and especially for the young and for women. We can’t rule out kids5.
The one thing we know that works against Long COVID’s CFS is vaccines. They probably reduce the danger of COVID’s CFS by 75-90%.
If you’re young and think “vaccines are not worth the risk” because your likelihood of dying was so low, consider that your likelihood of developing COVID CFS is about 3,000x higher than suffering from a bad vaccine side effect6.
Chronic Fatigue Syndrome is probably the most concerning aspect of COVID. If you have it, I am really sorry for you. So far, we’ve talked mostly about its deaths, but as deaths plummet thanks to vaccines, we have to start talking about this too since it affects young people who might not get vaccinated because the risk of deaths is not for them. The world is about to suffer the burden of millions of new CFS patients because of Long COVID. We need to limit that as much as we can.
Personally, I will remain vigilant: vaccines up-to-date, masks whenever I’m with lots of people, avoid long indoor events with crowds… I hope you do the same. Best of luck.
If you think somebody might benefit from reading this article—for example a young person or a woman who doesn’t want to get the vaccine—please forward it to them. The rest of their lives might depend on it.
There’s a lot of data in this article, based on many different papers collated together. Lots of it is imperfect, but we have to make do. Please take it with a grain of salt and always check for yourself. I very much hope to be wrong, and if data appears to say so, I will update you. Let’s hope for that.
Meanwhile, COVID CFS looks very bad, but unfortunately it’s not the only bad thing about Long COVID. I couldn’t cover the rest in this article: it’s already too long. The premium article this week will focus on the other worrying aspects of Long COVID:
Unregistered deaths
Post-Intensive Care Syndrome
Chronic loss of smell
…
I will also cover the most frustrating part: there have been many precedents of post-viral CFS, including the epidemic of a CFS-like illness just after the 1918 flu crisis. Sign up to the premium newsletter to read it.
I’m making several big assumptions here: one is that the chances are indeed 5% per child. The other is that there is no correlation between them: one kid developing it doesn’t increase the likelihood that another develops it too. Since it looks like there’s a genetic component to CFS, this is probably not true, but it is on average. So one family might have 0 of 4 kids with CFS and another one might have 2.
My short for “the type of Long COVID that looks like Chronic Fatigue Syndrome
This article describes how Ampligen might work for up to ~40% of traditional CFS. The drug is not approved yet, though, and their Phase III trial didn’t show an improvement over the control group. But Phase II did. The company behind Ampligen reported a positive Phase I trial for Ampligen on COVID, but I couldn’t find anything else.
The Karnofsky Performance Scale assesses this in patients. A perfectly healthy person gets a hundred on the scale, and a dead person gets a zero. The scores of patients with C.F.S. fell as low as thirty. Reference.
I’m taking a 2% chance of COVID CFS and a 1/150,000 chance of suffering some side-effect from vaccines. I go into a lot of detail on side effects and odds in this article.
Thanks - excellent article. I'm interested in how the symptoms of Long Covid as described above (CFS) interact with the generalized organ and system damage reported. So for example - is shortness of breath an effect of something like CFS, or is it lung/heart damage; or is it some combination? Even before being vaccinated, and being 60+, Long Covid seemed like far more of a worrying risk to me than death, but it was hard to get it through the heads of anti-vaxxers (I live near the epicenter of anti-science anti-vax conspiracy thinking in Australia) to think in terms of a significant chance of long-term constraints to their future freedom - to exercise, and live a normal life, rather than a low risk of dying.
This is a good article.
The only thing that's missing is the "why do we know so little about Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)?
(Please do not stop digging because of complexity)
Follow the money.
ME/CFS is the most underfunded disease to disease burden.
Despite a disease burden that is Double HIV with no treatment, funding at the NIH is only 7% of disease burden. The story is the same no matter which government in the world you choose. In the US, 13 Million dollars a year, for a disease that is having an economic impact of 51 Billion dollars a year.
"A study focusing on the disease myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), ∼75% of whom afflicted are women,2 found that disease to be the lowest funded (relative to disease burden) in the National Institutes of Health (NIH) portfolio.3,4 In carrying out the ME/CFS study, it was observed that some of the lowest funded diseases relative to disease burden were ones that affect primarily women. " (Mirin, A July 2021 https://doi.org/10.1089/jwh.2020.8682)
ME/CFS has been psychologized, meaning that money that could have been spent on biomedical science to find a diagnostic test, and treatments to slow progression of the disease have gone elsewhere.
Dr's are not educated to diagnose it, and treat the symptoms that can be treated which is part of the reason why suicide rates are so high (7 times normal population.
If you are a healthy, able bodied person who read this, please consider organizing a run/walk/bake sale for charities like Open Medicine Foundation which is leading the way in biomedical science for ME/CFS.
Thank you for your time.