
Should You Vaccinate Your Kids?

Kids are much less likely to die from COVID than older people, and vaccines have side-effects. So is it worth vaccinating them? Authorities tell you to do it. But their incentive is to stop COVID across the whole population, not just your kids. They might care more about kids spreading the virus to other people than about protecting them. So we can’t take their request at face value.
Which one is it, then? Are kids better off with or without a vaccine? The answer can be summarized in seven words.
Did somebody send you this article? Subscribe to receive future Uncharted Territories articles.
Vaccine Costs vs Benefits
When you assess a vaccine, you’re comparing the side-effects of the vaccine (costs) against the diseases caused by COVID (the benefit of the vaccine is the reduction of these diseases). This tradeoff is what we need to understand for each type of child.
Because “kids” means different things. You have males and females; infants, toddlers, kids, adolescents; healthy children and those with comorbidities; previously infected and naive… They react differently to both the vaccines and COVID.
You also have different vaccines, and different COVID variants. Pfizer is not like Moderna. Meanwhile, studies of COVID on kids from early in the pandemic might underestimate the virulence of Omicron.
And you also want to consider the risk that infected children cause: if a child won’t die of COVID but will infect grandma, who will then die, that’s something worth weighing.
One thing that humans also fear is the fact that you’re definitely risking vaccine side-effects once the needle goes into your arm. But you might or might not get COVID. However, with Omicron, we can’t assume that anybody is safe. We have to assume everybody will get exposed to it at some point. Especially with Delta’s and Omicron’s R0 of ~61. And now it’s clear that kids get infected as frequently as older people. That makes the calculations easier: we can just compare vaccine side-effects with COVID effects, without taking into account probabilities of catching the virus.
So in summary we need to look into:
The effects of COVID on kids
The side-effects of each type of relevant vaccine
For each segment: age, gender, health status
Correcting for other factors such as virulence of newer variants
Let’s do it.
Effects of COVID on Kids
The worst possible effect is death, so we need to take that into account. But it’s not the only one. Others include hospitalizations (never nice to see your child in the hospital), going to the ICU, the consequences of going to the ICU, PIMS (Pediatric Inflammatory Multisystem Syndrome2), and Long COVID.
There’s a bunch of numbers here, but don’t worry; I will summarize them.
Hospitalizations, ICUs, and Death
There have been about 800 deaths of children from COVID in the US so far. By May 2021 in Germany, there had been about 14.
Most of the data I have gathered below comes from a good German study from the end of November 2021, which looked at anyone below 18 years old. About 11% of German kids had built some natural immunity by May 2021—meaning they had probably been infected (or exposed) at some point.
The good news is that the estimation of the death rate of COVID on kids is on average 1 in 100,000 there. That means that if 100,000 kids get COVID, one will die. Hospitalizations and ICU admissions are much more frequent:

So 0.36% of kids with COVID will be hospitalized. That’s about 1 in 280 kids with COVID. What does that look like?

When this happens, your kid will be put into an isolation room where he is monitored. Most of the time, it will just be with some oxygen support. About 1 in 6,000 children with COVID will be admitted to the ICU (5% of those hospitalized). The worst ones might get hooked up to a ventilator, a dialysis machine, or something else.
Going to the ICU is quite a bad sign. 1 in ~10 won’t make it3. Those who do might end up with something called PICS, post-intensive care syndrome.
Post-Intensive Care Syndrome (PICS)
Here is how I explained PICS in The Other Long-Term Effects of COVID (emphasis added now):
When people spend a ton of time in the ICU, intubated, motionless, sometimes for weeks, at the edge between life and death, they tend to acquire chronic conditions. From this paper:
80% of ICU patients who survive up to 2 years after discharge are readmitted for care.
47% of ICU survivors at 2 year follow-up reported anxiety and depression.
Further deterioration of chronic pain and general health over 2 years.
31% of them experience major occupational changes, 25% become completely jobless.
33% can’t drive after one year.
This is called post-intensive care syndrome (PICS), which is well-studied. We understand the causes, and we know what happens to these people over time.
PICS might be connected to ARDS, “acute respiratory distress syndrome”, a form of pneumonia involving severe inflammation of both lungs:
“Many studies have shown that for some individuals, ARDS can have myriad long-term effects, including physical and cognitive impairments, reduced lung function, mental health problems, and poorer quality of life. A 1999 study found that even patients with less-severe forms of pneumonia can have symptoms that linger for months.
In addition, lung failure can precipitate the failure of other organs, like the kidneys and the heart, and can sometimes require specialized rehabilitation and care for months, or even years. SARS-CoV-2 infection can also (though rarely) inflict permanent damage on other organs, including severe myocarditis (an inflammation of the heart muscle leading to heart failure) and stroke, in the absence of significant lung disease.” StatNews
Put in another way: If you do go into the ICU, you will probably suffer a lot afterwards.
There’s not a lot of data for PICS in kids, but if you apply these PICS numbers to children going to the ICU, you get ~1 in 16k children infected with COVID who will end up with PICS4.
Pediatric Inflammatory Multisystem Syndrome (PIMS)
Days or weeks after a COVID infection, some kids will develop PIMS, Pediatric Inflammatory Multisystem Syndrome, whether they were hospitalized or not.

What’s PIMS5? The immune system might overreact and create inflammation across the body. Kids will develop a fever and maybe other symptoms like rashes, fatigue, weakness, tummy pains, headaches, red eyes, swollen hands and feet, peeling skin on hands and feet, diarrhea, vomiting…
~2% of kids with PIMS die, and ~15% have sequelae such as aneurysms and other dysfunctions. The rest return to normal.
Both PIMS and PICS deaths are usually not accounted for in the COVID fatality rate numbers, since kids have lost their COVID by the time they die6. Which means COVID deaths reporting is probably underestimated by ~10-20%7.
Here’s a key additional point: PIMS frequently includes myocarditis, about 75% of the time8.
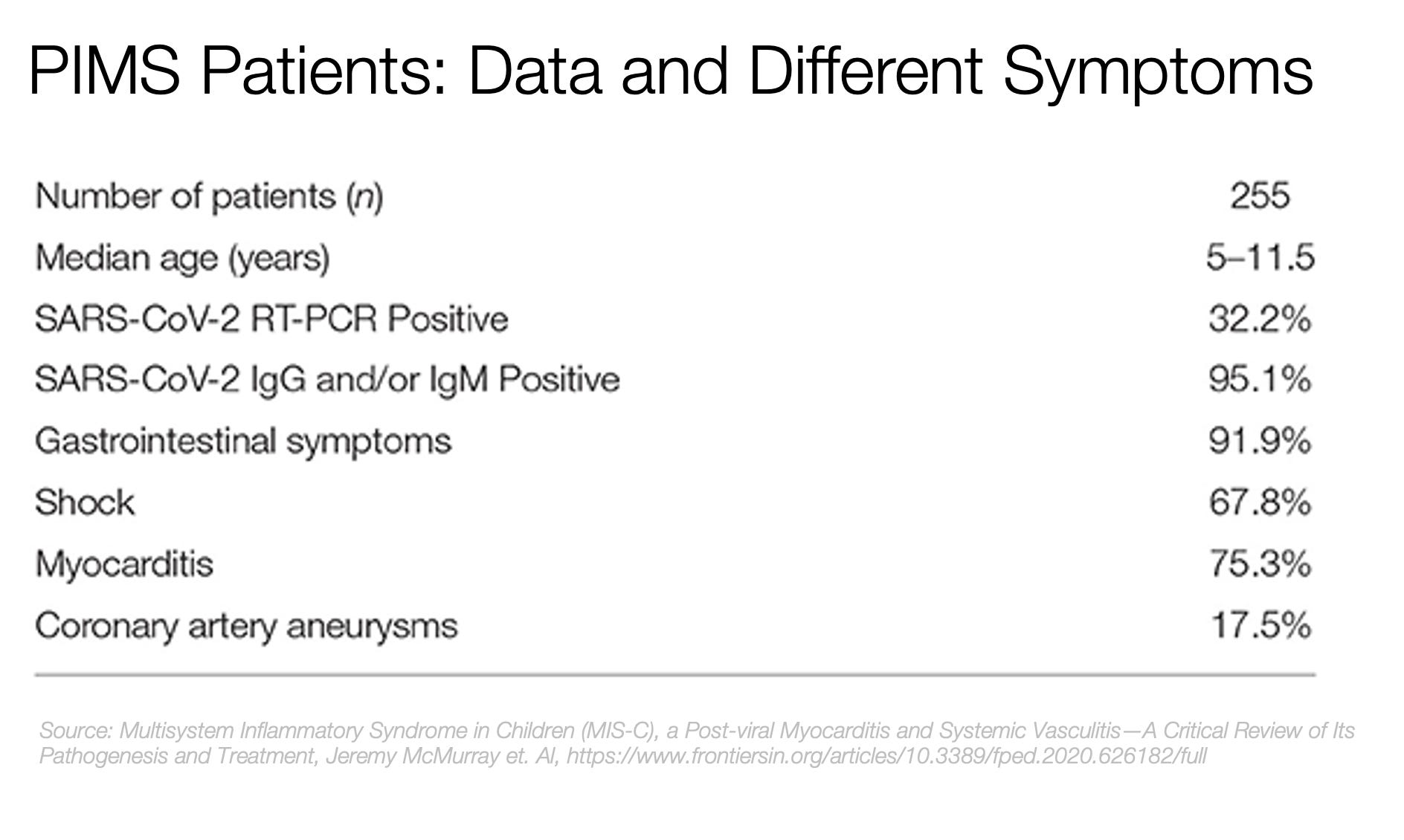
That puts COVID-related myocarditis at about 18 per 100k infections, or 1 in ~5k.
All of this is relevant, since as we’ll see later, myocarditis is the main concern with vaccines.
Long COVID’s Chronic Fatigue Syndrome
When thinking about the risks of COVID, most people only pay attention to deaths. They don’t pay attention to Long COVID because death is a big-enough risk. This is not true for young people, so it becomes important to take Long COVID into account.
PICS and PIMS fall into the category of Long COVID: symptoms that last for weeks after the main COVID infection subsides. Of all the bad Long COVID things you can get, one of the worst is Chronic Fatigue Syndrome (CFS)9.
I wrote an entire article on Long COVID focused on CFS. Read it if you want more details. Quick summary: CFS is super bad, you wouldn’t wish it on anybody, least of all your child. It has the potential to sap their energy for the rest of their lives. And there is no known cure. It’s probably linked to the virus lingering in the system or your immune system gone awry. We don’t know.
Here’s the prevalence of CFS for COVID infected people:

For kids 0-9, the risk is about 40 in 100k (or 1 in 2,500). For kids 10-19, it is 200 in 100k (or 1 in 500).
It’s slightly higher for teenage females:

Other COVID Effects
Kids can also suffer from strokes, blood clots, etc. I detail all of these side-effects in Other Long COVID Effects.
In summary, the worst things that can happen to kids are hospitalizations, ICU, PICS, PIMS, Chronic Fatigue Syndrome, and death. The numbers are pretty low though, ranging from 0.36% for hospitalizations to 0.001% for deaths (or 1 in 280 to 1 in 100,000).
How do these effects change with different factors, such as age and pre-existing conditions?
What’s the Effect of Age?
One interesting thing is that kids below 5 years old were 2-5 times more likely to die than older kids, suggesting that they might need to be vaccinated first. The death rate for kids below 5 was 1 in 50,000, whereas for kids 12-17 it was 1 in 250,00010.

Unfortunately, we test vaccines going from adults to younger and younger kids, to adapt dosages and make sure we don’t hurt the little ones. The downside is the vaccine arrives to them later, and some will die in the interi11m.
What’s the Effect of Comorbidities?
Healthy kids are as likely to be hospitalized as those with comorbidities, and over twice as likely to get PIMS. However, ICU and death are much less likely. 1 in 300k healthy children will die of COVID, whereas 1 in 40k of those with comorbidities will die (nearly 10x).

One thing to note: not a single healthy kid above 5 had died of COVID in Germany by May 2021.
In general, kids below 5 were the most at risk. 1 in 100k healthy ones died, and 1 in 25k of those with comorbidities.
PIMS, however, was quite common, didn’t change much across ages, and healthy kids were 2-3x more likely to develop it than those with comorbidities. 1 in 3k healthy kids developed PIMS.
How Does Omicron Change things?
A lot of the data above is based on the original variant or on Alpha. However, we know that Delta is 2x as virulent as Alpha. And as you know, despite what people say, it’s unclear whether Omicron is more or less lethal than Delta.
What this means is that all the numbers above might need to be doubled or so, to adjust for Delta virulence. Also, since Omicron has immune escape, vaccines might work less against it. Double the virulence from Alpha, plus much more immune escape, means Omicron’s lethality might be much higher than we think.
The Risk of Kids Spreading COVID to Others
Early on in the pandemic, we thought kids didn’t spread COVID much. But of course, early on in the pandemic, schools were closed, kids didn’t leave home much, didn’t get infections from outside, and hence didn’t infect other household members much. They appeared to “not be infectious”. When they did infect others, it was seldom realized they were the ones bringing the virus home, because they were less likely to have hard symptoms and be tested, so people didn’t realize they had caught COVID before other family members.
Now we know that kids do spread the virus, and wherever schools open, they’re more likely to catch it and spread it to family members. For the first variant, about 25% of kids infected adults in the household. The rate for kids below 8yo was 40% higher than for adolescents.
This is worth considering when you debate whether to vaccinate your kids.
Effects of Vaccines on Kids
The only vaccine approved so far for kids in the US is Pfizer, so that’s what we’ll study12.
Protective Effects of Vaccines
Kids 5-11 have the same antibody response to the Pfizer vaccine as those 16 to 25 years old. In the wild, outside of a clinical trial, the vaccine reduced the likelihood of infection in the children of this clinical trial by 91%.
Kids 12-18 are 93% less likely to be hospitalized with 2 doses of Pfizer. It looks like Moderna’s vaccine is going in the same direction.
Vaccines reduced PIMS in French adolescents by 90%.
Put in another way, it looks like for kids 5 and above, vaccines reduce infections and hospitalizations by ~90%. Our best bet is to assume they reduce other COVID diseases (PICS, PIMS, CFS) by at least the same amount13.
Side-Effects of Vaccines
In COVID FAQ 2, I explained how the main concern with vaccines for adolescents was myocarditis / pericarditis, which mostly affected males, at 1 in 30k cases, and no deaths. There’s much more data now. In the US, 1 in 16k cases for boys 12-17, and 1 in 150k for girls.
No other relevant side-effects have been identified.
From another study:

As a reminder, myocarditis from COVID in PIMS is 1 in 5k, so 3-30x worse than vaccine-triggered.
How do these two myocarditis compare? According to this study, vaccine myocarditis are mild:
“[This study] revealed relatively mild characteristics that subsequent research confirmed: Chest pain and shortness of breath are the most common symptoms, sometimes accompanied by a fever. Treatment includes ibuprofen for pain and sometimes steroids or a drug called IVIG that boosts the immune system. Hospital stays typically last a few days, primarily for monitoring. Most teens who develop post-vaccine myocarditis probably don’t need hospitalization, but since the phenomenon is new, most clinicians err on the side of caution.
We know this because we’ve been vaccinating kids for months now, so we have real-world data. We don’t have such data for kids 5-11, so we don’t know yet the rate of myocarditis / pericarditis in the wild. What we do know is that, in the clinical trials, no relevant side-effects were identified.”—Tara Haelle, The real risk of heart inflammation to kids is from COVID-19—not the vaccine, National Geographic.
From a study across 26 clinical centers:
Nearly 18.7% [of myocarditis cases in young people following a vaccine] had at least mildly decreased left ventricular function (squeeze of the heart) at presentation, but heart function had returned to normal in all who returned for follow-up.
Now compare that with the myocarditis from PIMS, when children catch COVID:
“What most pediatric cardiologists agree on is that cardiac complications seen with PIMS are more serious than the myocarditis seen from the vaccine.
Though nearly all children who suffered cardiac problems connected to PIMS have since recovered, the long-term effects remain unclear. Some children with PIMS get coronary artery aneurysms, in which a coronary artery widens well beyond what’s considered normal, says Jacqueline Szmuszkovicz, a pediatric cardiologist who specializes in PIMS at the Heart Institute at Children’s Hospital Los Angeles. Though rare, these aneurysms can sometimes be fatal. They also require long-term follow-up, possibly until adulthood, since they may affect a child’s future risk of coronary artery disease, Han says. Importantly, these aneurysms have been seen with PIMS but not with the vaccine.”—Tara Haelle, The real risk of heart inflammation to kids is from COVID-19—not the vaccine, National Geographic.
Now from the Scientific American:
Myocarditis can also be triggered by infections including COVID, which is far more likely to do so than vaccines are. Moreover, COVID-related myocarditis symptoms are usually much more severe than those seen in vaccine-related myocarditis, with the former leading to an average hospital stay of six days instead of one, she says. Infection-related myocarditis often requires lifesaving interventions such as medicines that help keep the heart pumping, or even a heart-lung bypass machine—and such cases often result in lasting heart damage.
All of this is for children 12-17. What about younger kids?
So far, five million American children ages 5-11 have been vaccinated (one million with two doses). No reported myocarditis.
The vaccine is not approved for children below 5 yet, but so far in clinical trials I am yet to see important side effects for them.
Oh, also, spacing the shots matters. If the two shots are taken within 30 days, the rate of myocarditis is 5x higher than if they’re spaced by 60 days or more. Just space the shots by 2-3 months instead of 2-3 weeks to be much safer.
Finally, Moderna protects better, but it also has more myocarditis. This finding has been confirmed in the US, Canada, Japan, Germany, France, and in other Nordic countries. If you’re scared of myocarditis, take Pfizer.

Long-Term Side-Effects
One of the main concerns about vaccines is long-term side-effects: we have only tracked people for a few months in clinical trials, and a few more months in the wild. How do we know it’s safe after a year? Five years? Twenty years?
If this is your concern, you will probably have heard this response: “Yeah but most vaccine side-effects happen within weeks or a couple of months of the injection.” Is this true?

Most of the serious side-effects identified in vaccines have appeared within weeks of the injection.
Any time there’s been a serious concern about long-term consequences of a vaccine, it’s been studied:
Dengue is usually mild the first time and more aggressive the second time when infected by a different strain. The Dengue Fever vaccine can act as a first infection, so an actual Dengue infection can be interpreted by the body as a second infection and the recipient might have a more intense reaction than if he hadn’t received a vaccine. But that didn’t entail chronic conditions.
There was a concern that children's vaccines could cause diabetes later on, but a meta-analysis ruled that out.
There was a concern that vaccines could make people develop multiple sclerosis. A literature review was inconclusive for the BCG vaccine, and concluded that vaccines for hepatitis B virus, human papillomavirus, seasonal influenza, measles–mumps–rubella, variola, tetanus, Bacillus Calmette-Guérin (BCG), polio, or diphtheria didn’t increase multiple sclerosis.
Subscriber Regitze I. tells me that a specific brand of H1N1 vaccine, Pandemrix, gave a higher risk of narcolepsy in specific countries, which may be linked to local genetics.
As for COVID vaccines, they’ve been around for one year now, and countries around the world have been monitoring side-effects. No long-term ones have been discovered so far. Yet we know the system works, since we caught the blood clots from J&J and the myocarditis from mRNA vaccines14. I am not worried about long-term side effects.
What Do Governments Say?
Most governments are approving the vaccine for kids. The one I could see that disagreed was the UK Government. This is their summary of the data, for healthy children:
“Overall, the committee is of the opinion that the benefits from vaccination are marginally greater than the potential known harms (tables 1 to 4) but acknowledges that there is considerable uncertainty regarding the magnitude of the potential harms. The margin of benefit, based primarily on a health perspective, is considered too small to support advice on a universal programme of vaccination of otherwise healthy 12 to 15-year-old children at this time. As longer-term data on potential adverse reactions accrue, greater certainty may allow for a reconsideration of the benefits and harms. Such data may not be available for several months.”—UK Joint Committee on Vaccination and Immunization (JCVI).
Either the US CDC is wrong, or the UK JCVI is wrong. Which one is it? So far I agree with the CDC, so I looked into the JCVI’s opinion. Here’s why they say this.

The first thing to note is that the orders of magnitude are different from those before. The UK reporting is ~10x lower than for Germany. That is to be expected, because the German reporting structure is quite different from the UK one. Here, what we should pay attention to is orders of magnitude.
The UK basically says that if a vaccine gives you myocarditis, it might not be worth it for averting ~30x as many hospitalizations, ~1-5x the rate of PIMS, and ~0.1-1x the rate of PICS. Here’s what they’re missing:
They forgot the myocarditis that comes from PIMS! Which, according to these numbers, is ~1-5x more common than from the vaccine15.
They didn’t account for the severity of COVID-related myocarditis coming from PIMS.
They did not account for Chronic Fatigue Syndrome.
They don’t realize that most of the benefit of the vaccine is in the 1st dose, but it’s only 25%-50% of the cost, which means a first dose would be very sensible.
And they don’t address these points in the report. They’re just left out. Maybe not considered.
What they do address is that they don’t want to take into account social benefits of vaccination (kids infecting others), which I understand. But that’s another miss. Instead, they could present it like: “Pros and cons are both very low, but the risk of children infecting others is high. You might weigh that when considering whether you want to vaccinate your kids or not.”
What About Anti-Vaxxers?
I looked into their arguments. It’s a lot of work to track every point down, so I did this in the premium article of this week. Sign up to get it. The high-level takeaway is that I still reach the same conclusions, but I disagree with our treatment of misinformation.
Putting It All Together
In kids, the Pfizer vaccine reduces the odds of myocarditis by ~3x and makes it milder1617. That, right there, should be enough incentive to vaccinate kids.
“The pediatric hospital experience shows that the risk of patients at any age having cardiac involvement from COVID is uniformly worse than vaccination myocarditis risk.”—Frank Han, pediatric cardiologist, OSF Healthcare, Central Illinois.
And then, on top of that, it reduces deaths, hospitalizations, ICU stays, PICS, PIMS, and CFS18:
It 10x reduces infections.
It 10x reduces hospitalizations, from 1 in 280 to 1 in 2,800.
It probably reduces the rest of consequences by a proportional amount. Which means:
Deaths would go from ~1 per 100k to ~1 in 1 million.
PICS would be reduced from 1 in 16k to 1 in 160k.
PIMS would be reduced from 1 in 4k to 1 in 40k.
CFS would be reduced from 1 in 500 to 1 in 5,000 (10-19) and 1 in 2,500 to 1 in 25,000 for 0-9.
All these numbers should probably be doubled given Omicron is likely more virulent than the original variant / alpha, and has a lot of immune escape. Meaning for example the risk of PIMS might not be going from 1 in 4k to 1 in 40k, but rather from 1 in 2k to 1 in 20k.
Vaccination also probably reduces the infection of other people in the household. Kids spread the original variant in about 25% of households. Probably more with Delta / Omicron. Vaccines reduce Delta infections by 50%, so if we take that number as an order of magnitude, you’d go from 25% of kids infecting adults in households down to ~10-15%.

Depending on your kid, there are some nuances:
If your kid has comorbidities, it’s a no-brainer: the vaccine will prevent their death and other things, such as PICS, PIMS, CFS… All of these are quite bad and you want to protect your kids from them.
If your kid is healthy and older than 12 years old, the odds of death from COVID are very, very low. However, vaccines will protect them from PIMS (including myocarditis), PICS (including myocarditis), or Long COVID, and will reduce their myocarditis
If she is healthy, older than 12 years old, and a female, it’s even more of a no-brainer, since the risk of vaccine-induced myocarditis is about 5x lower.
If your kid is healthy and between 5 and 12 years old, they’re not likely to die of COVID, but it's still possible they'll develop PIMS, PICS, or CFS. We have clinical trials telling us that the vaccines are safe for them, and now one million of these kids vaccinated in the wild with no serious side-effects. I have two kids in that category. I will vaccinate them as soon as I can.
If your kid is healthy and below 5 years old, you can’t vaccinate them yet: vaccines haven’t been approved. But from what we know today, vaccines are probably safe for them, and probably prevent COVID deaths, which is important since this group has more risk of death. With what we know today, it’s a no-brainer to vaccinate them once vaccination safety is confirmed.
If you’re on the fence, here are some additional thoughts to consider:
The first dose is much more valuable than the second dose, while the second dose has more side-effects. If you are in doubt, just give the first dose and then wait and see.
Spacing also matters. If the two shots are taken within 30 days, the rate of myocarditis is 5x higher than if they’re spaced by 60 days or more. Space the shots by 2-3 months instead of 2-3 weeks and you should be good.
Also, Moderna appears to have more myocarditis than Pfizer, which might be why Pfizer is approved for kids and Moderna isn’t yet in the US. In Denmark, that rate was 3x. In Canada, 5x. So just have your kid take Pfizer19.
I started this article not knowing whether I should vaccinate my kids. But it turns out the worst side-effects of vaccines are mild myocarditis—mostly 12-17 year old males—and there have been no deaths from mRNA vaccines in kids. Compared to all the bad stuff that COVID can do to kids (death, PIMS, PICS, CFS), including more common and worse myocarditis than with vaccines, I think the answer is clear based on the data we have: you should vaccinate your kids. I will definitely vaccinate mine.
Do you know people with kids? Associations, schools, groups of parents who might be interested in knowing what to do with their kids’ vaccinations? If you thought this article was relevant to them, send it to them!
And if you haven’t yet, subscribe to this newsletter for more articles.
One infected person can infect 6 other people. Current approximation for Delta, guess for Omicron.
Sometimes you can see it as PIMS-TS. AFAIK, the TS stands for “temporally associated with SARS-CoV-2 infection”
The numbers are quite low, so it’s hard to tell these things. The German data says 1 in 18, but in another source it’s 1 in 6. The point is not precision, it’s about orders of magnitude.
I couldn’t find the rate of myocarditis for kids in PICS, so I won’t consider it. But I wouldn’t be surprised if it was sizable.
Sometimes known as PIMS-TS or MIS-C
I haven’t seen this explicitly mentioned, but it’s usually true for adults, so unless I’m told otherwise I’ll assume it’s true for kids.
Given the orders of magnitude we’re talking about, 10-20% is not a huge deal. There are many other more important sources of underreporting. For example, what if a kid has developed PIMS but is not tested for COVID? Case underreporting is probably a bigger source of error here.
To qualify for the PIMS diagnosis, more than one organ needs to be involved. Which means that looking at myocarditis from PIMS is going to underestimate the prevalence of myocarditis…
Different sources have different assessments of Long COVID prevalence. But many have an agenda, which might try to increase or decrease your fear of Long COVID. Some might suggest half of kids will have Long COVID, but when you look at the fine print they mean some symptoms a few weeks after the disease. If we start taking into account all these symptoms, we lose the big picture. So instead we need to focus on the ones that matter. For Long COVID, the problems are PICS, PIMS, and CFS. But PICS and PIMS are short term. The main concern of long-term Long COVID is CFS, because it’s super debilitating and might be life-long. The prevalence of that is much lower than all of Long COVID, so beware when people suggest otherwise.
All these numbers are so low, even for a country like Germany with 14 million children in this study, that these numbers should be taken as ball-park figures. For example, when we say 1 in 50,000, it could be 1 in 25,000 or 1 in 150,000. But it won’t be 1 in 10,000,000 or 1 in 1,000.
Also, note that kids 5-11 were the safest of them all up to the ICU level. I assume the fact that deaths appear higher for that group is because the sample size is too small—which tells you something: when out of 14 million kids, the deaths don’t have a big enough sample size…
Pfizer tested 30 micrograms of vaccine for kids 12-18, 10 micrograms for kids 5-11, and 3 micrograms with kids below that. The 3 micrograms one is not enough for kids 2-5, so they’ll add a booster or increase the dosage.
In adults, COVID vaccines protect more the closer you are to death. Eg, vaccines reduced Delta infections by only 50% but hospitalizations and deaths by ~90%.
Some anti-vaxxers fear that all of this is not enough evidence, because there are precedents of medication causing long-term side-effects. I’ll address this in the premium article later this week. Sign up to get it.
If you keep assuming 75% of PIMS includes myocarditis
Here’s your seven-word summary: vaccines make myocarditis less frequent and milder.
Remember that PIMS is more frequent in healthy kids than those with comorbidities, so myocarditis for healthy children is still more likely from PIMS than from the vaccine.
Using the Germany data here for consistency.
That said, risks are low, so this is actually a low-stakes individual decision (but a very high-stakes social decision). If you lean either way, that would make sense.
The UK JCVI statement you discuss was about vaccination for ages 12-15. The JCVI recognized a benefit, so it is unlikely that the additional considerations you give would change the calculations much, particularly as it had not been demonstrated that the vaccine reduces the risk of PMIS, if infected. However, there is not necessarily a big difference between the JCVI's and your views. The JCVI recognized that there may be other considerations that strengthen the case for vaccination, and explicitly suggested the Chief Medical Officers consider those in making their final recommendation. The decision of the CMOs at that time was to make one dose of vaccine available, recognize that there should be no stigmatization of parents who choose not to vaccinate due to the fine balance of arguments, and state that the issue of a second dose should be revisited in a few months. Those decisions were before Omicron emerged. When Omicron emerged, the UK decided to give second doses for ages 12-15.
Excellent post. Can you draft an essay on the efficacy of booster shots?